

Abstract
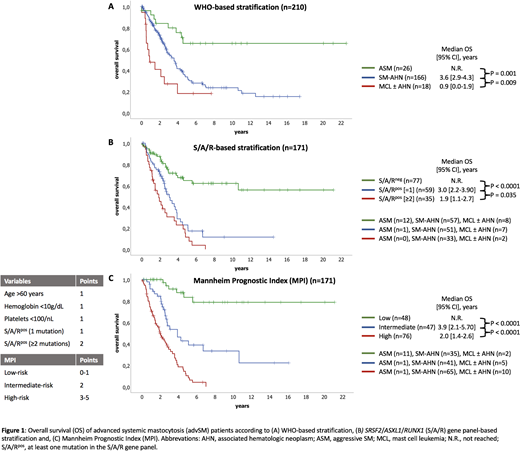
According to the WHO classification, advanced systemic mastocytosis (advSM) comprises aggressive SM (ASM), SM with an associated hematologic neoplasm (SM-AHN) and mast cell leukemia (MCL). SM-AHN is the most common subtype of advSM, diagnosed in up to 80% of patients. The AHN is characterized in >90% of patients as a myeloid neoplasm, e.g. CMML. Acquired mutations in KIT (usually KIT D816V) are detectable in >90% of patients. The SM-AHN phenotype is usually based on clonal involvement of KIT D816V in various hematopoietic lineages, e.g. monocytes, eosinophils and other non-mast cell lineages. However, recent data have highlighted that the molecular pathogenesis of advSM is much more complex and involves one or more additional mutations (e.g. SRSF2, ASXL1, RUNX1, S/A/R gene panel) in 70-80% of the patients. The presence of at least one mutation of the S/A/R gene panel (S/A/Rpos) has a strong adverse impact on disease phenotype, prognosis, and response to treatment, e.g. midostaurin (Jawhar et al., Blood 2017). With data from 210 advSM patients enrolled in the 'German Registry on Disorders of Eosinophils and Mast Cells', we evaluated a) clinical and genetic characteristics, b) treatment, c) survival and, d) developed a new prognostic score for advSM (Mannheim Prognostic Index, MPI). Subtypes of advSM included SM-AHN (n=166, 79%), ASM (n=26, 12%), and MCL ± AHN (n=18, 9%). Median age was 69 years (range 18-90, 67% male). The median MC infiltration in the bone marrow by histology and immunohistochemistry was 30% (range 5-100) and the median serum tryptase level was 168 μg/L (range 13-1854, normal value <11.4 μg/L). Relevant blood parameters included: hemoglobin (median 10.3 g/dL, <10 g/dL in 46% of patients), platelets (median 118x109/L, <100 in 42% of patients), monocytes (median 0.6x109/L, >1.0 in 34% of patients), eosinophils (0.3x109/L, >1.0 in 30% of patients), alkaline phosphatase (median 179 U/L, >150 in 58% of patients). Hypoalbuminemia (<35 g/L) was diagnosed in 36% of patients and splenomegaly in 84% of patients. Mutations in KIT were identified in 201/210 (96%) patients (D816V, n=195 [93%]; D816H, n=3; D816Y, n=2; F522C, n=1). In 171 (81%) patients, DNA for targeted next-generation-sequencing of recurrent myeloid mutations was available. In addition to KIT mutations, 141/171 (82%) patients had at least one additional mutation (median, n=2; range, 1-7). The most frequently affected genes (≥5%) included TET2 (n=70, 41%), SRSF2 (n=67, 39%), ASXL1 (n=36, 21%), RUNX1 (n=29, 17%), JAK2 (n=22, 13%), CBL (n=15, 9%), N/KRAS (n=15, 9%), EZH2 (n=9, 5%), IDH1/2 (n=9, 5%) and, SF3B1 (n=9, 5%). S/A/Rpos were identified in 94/171 (55%) patients. Cytogenetic analysis was performed in 154 (73%) patients and an aberrant karyotype was identified in 27/154 (18%) of patients. Treatment modalities included midostaurin (n=49, 23%), cladribine followed by midostaurin or vice versa (n=30, 14%), cladribine (n=21, 10%), and allogeneic stem cell transplantation (n=20, 10%). The median overall survival (OS) was 3.8 years (deaths, n=114 [54%], 95% confidence interval, CI [3.2-4.4]) for all patients and not reached (n.r.) for ASM, 0.9 years for MCL ± AHN, and 3.6 years for SM-AHN (Figure 1A). Overall, 33/210 (16%) patients with ASM (n=12) or SM-AHN (n=21) progressed to MCL ± AHN (n=14) or SM-AML (n=19) after a median time of 19 months (range, 2-70). Twenty-three of 31 (74%) of these patients were S/A/Rpos. In univariate analyses of multiple clinical, laboratory and molecular parameters, S/A/Rpos was the strongest predictor (hazard ratio [HR] 3.9 [2.4-6.3], P<0.0001) of an inferior OS (Figure 1B). In multivariate analyses, age >60 years (HR 2.4 [1.4-4.1], P=0.003), hemoglobin <10g/dL (HR 1.9 [1.2-2.9], P=0.005), platelets <100x109/L (HR 1.6 [1.1-2.5], P=0.03), S/A/Rpos (1 mutation) (HR 2.5 [1.4-4.2], P=0.001), and S/A/Rpos (1 mutation vs. ≥2 mutations) (HR 1.7 [1.0-2.4], P=0.01) remained independent poor-risk markers for OS. According to the HR, a WHO-classification independent, weighted (HR 1.6-2.5, 1 point) MPI for advSM was assigned: low-risk (0-1 points, 48/171, 28%, median OS n.r.), intermediate-risk (2 points, 47/171, 28%, median OS 3.9 years) and high-risk (3-5 points, 76/171, 44%, median OS 2.0 years) respectively (Figure 1C). Particularly, the SM-AHN and the MCL cohorts defined as intermediate- and high-risk according to the WHO-based stratification can be well stratified within the 3 MPI cohorts.
Meggendorfer:MLL Munich Leukemia Laboratory: Employment. Haferlach:MLL Munich Leukemia Laboratory: Employment, Equity Ownership. Valent:Pfizer: Honoraria; Incyte: Honoraria; Novartis: Honoraria. Reiter:Incyte: Consultancy, Honoraria.

